
Background
Rwanda has made tremendous progress in reducing the burden of malaria in recent years. Between 2015/17 and 2022/23, there has been a reduction in:
- malaria incidence, down from 409 to 47 cases per 1,000 population
- prevalence in children under 5 years, down from 7.2% to 0.6%
- deaths, down from 536 to 51 deaths
Several interventions and their strategic deployment have contributed to this success, including:
- sustained and evidence-guided vector control interventions, such as indoor residual spraying and introduction of new types of insecticide-treated nets such as PBO (pyrethroid-piperonyl butoxide) and IG2 (Interceptor G2) nets
- home-based management for early diagnosis and treatment of malaria by community health workers (CHWs)
- implementation of social and behaviour change (SBC) activities through civil society organisations (CSOs), local NGOs and faith-based organisations (FBOs)
- use of drones for larviciding
- improvement in routine surveillance, monitoring and evaluation and the use of data to guide implementation of interventions
- sub-national stratification to guide prioritisation of interventions
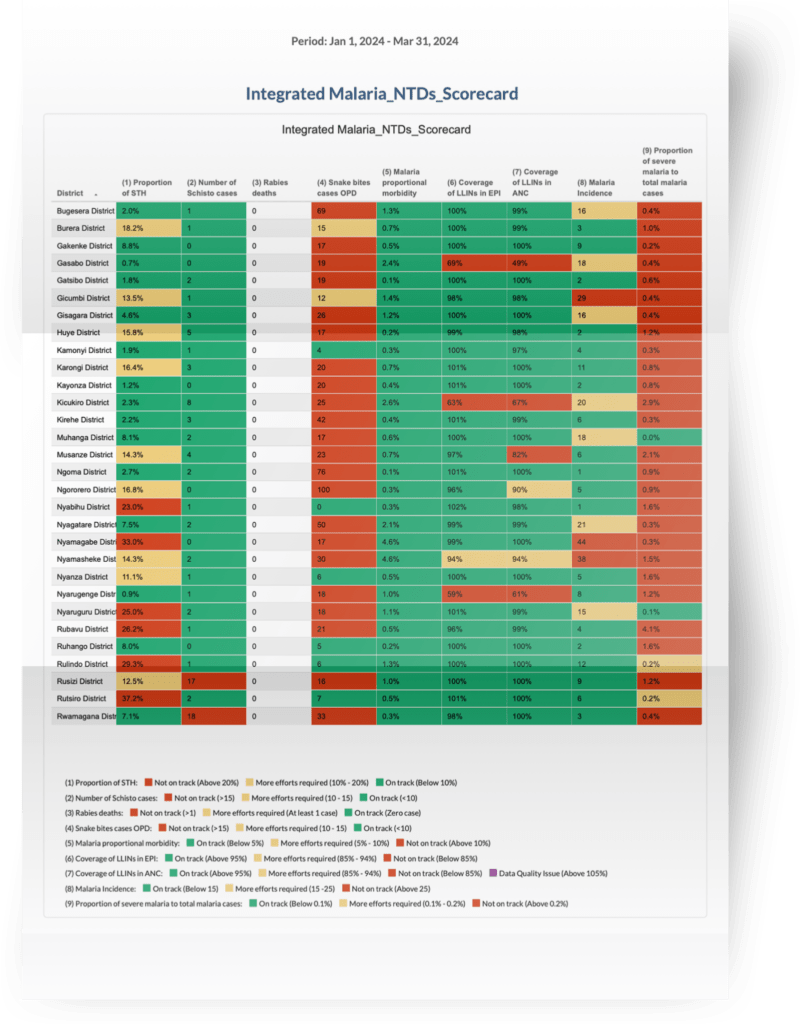
Rwanda’s malaria scorecard was developed in 2017. In 2019, indicators to address neglected tropical diseases were introduced into the scorecard for a more integrated approach to monitor progress made in disease control. The malaria and NTD scorecard is one of the main tools used by the Malaria and Other Parasitological Diseases Division (MOPDD) and its partners to routinely review progress and identify and address bottlenecks.
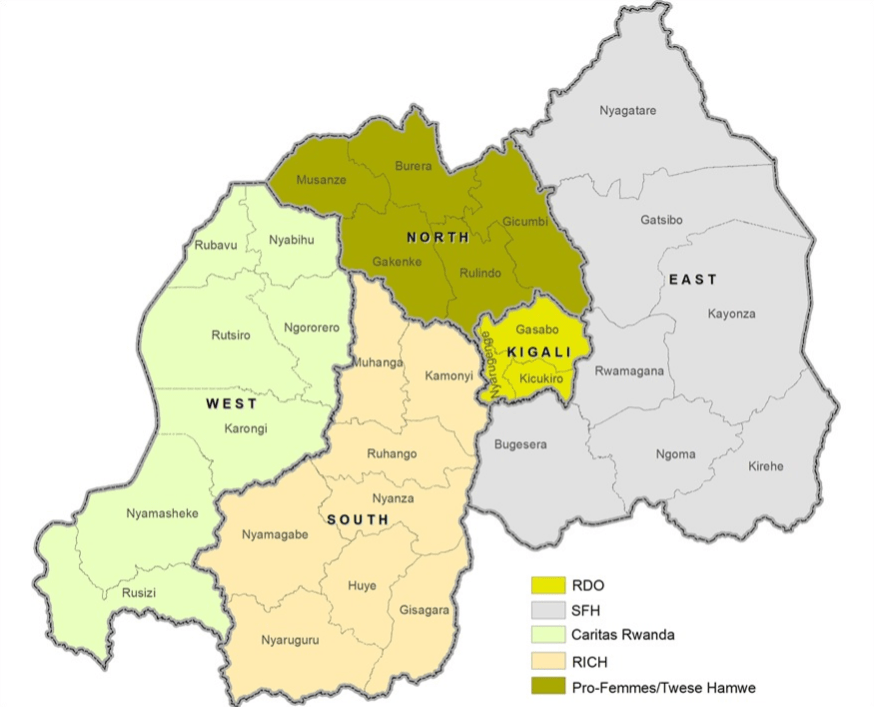
In 2020, the MOPDD trained members of five civil society organisations (CSO) in the use of the scorecard. The purpose of the training was to build capacity of CSOs in routine data use to guide planning, resource mobilisation, implementation of social behaviour change interventions and community mobilisation. The CSOs support malaria control implementation in all five provinces in Rwanda.
Each CSO is assigned to work in a province, including all its respective administrative areas (districts, sectors, cells and villages). CSOs are primarily responsible for conducting social behaviour change activities to support implementation and uptake of interventions at sector, cell and village levels.
Operationalisation of malaria and NTDs scorecard by CSOs
The MOPDD is responsible for populating the scorecard and sharing it every month with CSOs. At subnational level, the scorecard is also shared with district and sector health leaders, hospital and health facility managers and staff. The scorecard is reviewed with stakeholders at the different levels and corrective actions to address identified bottlenecks are agreed upon.
CSOs discuss the scorecard with community health workers (CHWs) and other actors at community level. Based on discussions in scorecard review meetings, CSOs request funds from the Ministry of Health, through the MOPDD, to implement actions to drive indicator improvement, mainly targeting sectors and underperforming indicators (in red on the scorecard) and those that still need further improvement (in yellow on the scorecard).
CSOs use the scorecard to agree on and undertake joint actions with community leaders and members, and local authorities. During monthly review meetings, progress against previous actions is assessed and new actions are triggered as needed. The scorecard is also used by the MOPDD to assess CSO performance and as such for strengthening accountability for agreed contracts, activities and focus.

Examples of community engagement and actions triggered by the scorecard
These are examples of community-level issues identified by the scorecard and addressed jointly by CSOs and communities with support from other stakeholders.
Addressing bednet misuse in Nyamasheke district
In May 2022, the scorecard showed six sectors in Nyamasheke district were underperforming for the indicator ‘number of malaria cases’. These were among ten sectors with the highest malaria cases in the country. On investigation it was found that insecticide-treated bednets (ITNs) were being used for fishing instead of protection against malaria, leading to higher-than-expected exposure to malaria infection.
In response, fishermen cooperatives were trained in the dangers of malaria and the importance of ITN use for prevention against infection. After this training, the cooperatives of fishermen supported by the Caritas Rwanda CSO, local leaders, health facility staff and security agencies, undertook an operation code-named ‘Operation Supanet’ to identify community members using ITNs for fishing, and educate them in proper ITN use. This activity was followed by community health worker home visits to check and advise on proper ITN use.
These efforts contributed to the decrease of malaria cases from 106 per 1,000 in the FY2021/22 to 76 cases per 1,000 population in Nyamasheke district.
Community management of mosquito breeding sites in Rubavu sector

An increase in the number of malaria cases at Rubavu sector in Rubavu district, was observed through the scorecard in 2022. Further analysis and discussion showed that the increase was attributed to stagnant water originating from Rubavu hill.
To solve this problem, the local population introduced ‘ISAHA Y’ISUKU’ (cleaning hour), conducted every Monday and Thursday from 7am to 8am in Byahi sector. Activities included work to:
- remove stagnant water
- sensitise community members on sanitation and hygiene activities
- sensitise community members on other malaria preventive measures including the proper use of ITNs
This practice was supported by Caritas Rwanda and adopted by all sectors in Rubavu district.
Establishing intersectoral collaborations to control breeding sites in Rubavu and Kamonyi districts
After raising awareness about the problem of water flowing from Rubavu hill and creation of mosquito breeding sites through water stagnation, the local government of Byahi sector and community members, supported by Caritas Rwanda, mobilised resources from households in five villages (Gafuku, Mubuga, Rebero, Kitarimwa and Karukogo) to construct community roads to improve water drainage and support wider development. The national government – through Rubavu district – contributed US$100,000 to the initiative to construct roads of up to 8.5 kilometres. There was an associated reduction in malaria cases from over 3,000 to 38 cases per month over three months.
Mugina sector in Kamonyi district had the highest number of malaria cases in the district for several months in 2022. Rwanda Interfaith Council for Health (RICH), the CSO responsible for implementing malaria social and behaviour change in the district – in collaboration with local leaders and health workers – conducted field visits to identify the reasons for high cases and found that there were many mosquito breeding sites around mines leading to high malaria exposure among mining workers.
Before this, we used to have challenges with many cases of people who would miss work because they were sick. This seriously affected our work, we then decided to make sure all our staff have this knowledge and also shared this with other members of our cooperatives working in the same field. With everyone’s commitment in practicing these positive behaviours, we are now happy to see that malaria is really being eradicated in this area.
Diane Mukakalisa, owner of one of the mining sites in Mugina sector
After being trained by RICH, the owners of the mining sites in Kamonyi shared the knowledge gained with their staff and advised them to educate their peers in order to motivate community action to eliminate mosquito breeding sites and practice other malaria preventive measures including the use of mosquito repellents at work. This action contributed to the reduction in malaria incidence below 100 cases per 1,000 in all sectors of Kamonyi districts in the financial year 2023/2024 compared to the financial year 2022/2023.
Conclusion
Rwanda is using the malaria and NTD scorecard tool to institutionalise data-led decision making and action at all levels of malaria control. The use of the scorecard by civil society organisations to identify community and sector-level bottlenecks and mobilise effective community and multisectoral engagement has resulted in high impact actions and outcomes. The use of the scorecard as a simple yet comprehensive tool to communicate the status of malaria control across stakeholders will continue to play an important role as Rwanda progresses towards malaria elimination.