Introduction
In 2014, Bungoma County in western Kenya had some of the lowest Reproductive, Maternal, Neonatal, Child and Adolescent (RMNCAH) outcomes and health inputs in the country. Yet maternal mortality rates (MMR) have declined by 25% in recent years while newborn mortality rates (NMR) are approaching the national target. How has this been possible? Though multiple factors have played a role, one important change in the County’s health system has been the implementation of the scorecard management tool. The Scorecard’s digital platform translates real-time health system data into a simple, easy-to-understand, color-coded format and makes it accessible to those who need it to improve health service investments and outcomes.
How it works
Bungoma County began rolling out the Scorecard in late 2017 and, within less than 2 years, remarkably has decentralized Scorecard review and use down to the sub-county, ward and health facility levels.
Every quarter, the Scorecard is a standing agenda item for both Ministry of Health (MoH) county performance review meetings and sub-county data review meetings. Facility-in-Charges attend the sub-county meetings and, though they do not yet have digital access to the Scorecard, the Health Facility (HF) officers participate in analysing their facility-specific Scorecards during the meetings and agree on follow-up actions. These actions are then entered into the RMNCAH Scorecard Action Tracker by the Sub-County Health Records and Information Officers (SCHRIOs). The County Health Management Team (CHMT) also holds regular performance review meetings in the presence of partners to review the scorecards and identify solutions which are then captured in the action tracker. The creation of an RMNCAH Task Force is being created to keep coordination and joint planning in response to the Scorecard strong between the government and partners, as well as to monitor implementation of tasks in the Action Tracker.
Bungoma is also the first county to fully utilize the Action Tracker functionality. The Action Tracker is a management functionality on the online scorecard web platform that allows managers to assign actions to individuals and track the progress of those actions as they are implemented. The system generates automatic SMS and email reminders until the action is marked complete. Action owners are responsible for coordinating and reporting on the progress of the action item, which can be monitored by anyone who has access to the system, thereby strengthening transparency and accountability. Though HFs in the county are not yet able to use the on-line Action Tracker, they update quarterly workplans to address areas of underperformance on the Scorecard.
The Scorecard is working. Once the Scorecard became available, it helped us regularize performance review meetings at all levels. The color-coded system and arrows displayed by the Scorecard really help motivate people to improve performance.
George Wanzala, Reproductive Health Coordinator, Bungoma County Health Department
Impact
Resource mobilisation
From 2017 to 2019, following consistent use of the Scorecard as an evidence-based advocacy tool by the CHMT and partners with the County Executive Committee (CEC), the County’s health budget increased by 27.5% from KSH 2.6 billion (~$26 million) to KSH 3.3 billion (~$33 million). In 2018, designated budgeting for RMNCAH services was done for the first time with KSH 55 million (~$550,000) earmarked in 2018 and KSH 51 million (~$510,000) in 2019.
Political commitment
The Scorecard is shared each quarter with Members of the County Assembly (MCAs), particularly MCAs who serve on both the Assembly’s Health Committee and the County Health M&E Technical Working Group (TWG). The County Executive for Health also expects to see the Scorecard on at least a quarterly basis and copies are printed by the CHMT-designated Scorecard Champions prior to all County Executive Committee (CEC) meetings.
Data quality
With demand for the Scorecard data growing in the county from senior government leaders, local politicians and major donors alike, there has been a resultant positive impact on data quality. Sub-County quarterly review meetings have been able to pinpoint wards and HFs with data reporting challenges and errors, which has led to targeted data collection and reporting capacity building in several areas. As reflected in the RMNCAH Scorecard Action Tracker this includes Vitamin A and improved reporting on long-life insecticide treated nets (LLITNs) for pregnant women and infants under one year. For the first half of 2019, Bungoma County HFs have performed at 100% in terms of timeliness and completeness of routine HMIS reporting.
Stakeholder coordination
Following introduction of the Scorecard, major health sector partners indicate stakeholder coordination has significantly improved. Partners, all of whom actively participate in the semi-annual Health Sector Stakeholder Forum, also have been given ‘Viewer’ access rights to the Scorecard web platform. The Scorecard is a standing agenda item at all Stakeholder Forums and Health NGO Network (HENNET) meetings. The creation of a County RMNCAH Technical Working Group (TWG) is also under discussion which is meant to provide joint stewardship between county government and partners of the programming aspects implicit in the Scorecard data and agreed actions.
Tangible service delivery improvements have been observed as a result of RMNCAH scorecard use
Strengthening birth companion and referral services.
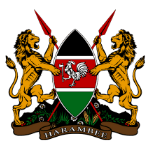
In Q2 2017 as the Scorecard was beginning to be used in the County, the Scorecard review showed skilled deliveries were just over 50%. This led to a focus by the county government and partners to improve this key indicator. One major response, with support from Options recently concluded MANI Project, involved the re-orientation of traditional birth attendants (TBAs) to become birth companions and referral agents for facility deliveries. Health workers from Primary Health Care (PHC) facilities were also provided with mentorships at the County Referral Hospital to learn more about how to handle pregnancy-related complications and when to refer. By Q2 2019, over 400 TBAs were retrained and supported more than 14,900 women to go to HFs for skilled birth assistance (SBA). Most birth companions also remained in touch with the new mothers at least through the first 6 months of the infant’s life to promote full immunization coverage (FIC) and other ante-natal best practices (4 antenatal care (ANC4) visits, use of LLINs to combat malaria, etc.)
Improving the availability of essential supplies at PHC facilities
Actions taken, as documented in the Action Tracker, include redistribution of key drugs commodities between facilities in Kanduyi and Webuye West Sub-Counties and earlier placement of drug orders in certain sub-counties to avoid stockouts, which is tied to continued improvements in ANC4, FIC and LLINs coverage (see below graph). Pressure was also applied on the CEC by the CHMT and partners to make full payment of arrears to the Kenya Medical Supplies Agency (KEMSA) so supplies orders could be released. Currently all PHC facilities in the county have all essential drugs and non-pharmaceuticals.
Increased full immunisation coverage (FIC)
From 2012-2016, FIC in infants was declining. Following Scorecard use and follow-on bottleneck analysis, actions were taken and recorded in the Scorecard Action Tracker, with support of partners including Save the Children International, SETH, E4A MamaYe and MANI Projects. These included intensifying defaulter tracing; ensuring all immunizing facilities offered daily immunization services; and improving documentation of both facility and outreach immunization data in four targeted sub-counties: Tongaren, Bumula, Webuye East and Kimilili.
Success story: Partners consider RMNCAH scorecard essential
Bungoma’s partners, including Evidence for Action (E4A) MamaYe3 project managed by Options, the Systems Enhanced Transforming Health (SETH) project co-managed by Action Against Hunger and Hellen Keller International, Save the Children, Palladium’s Tupine project, AMPATH, JHPIEGO and Jacaranda among others, said they have intensified their joint advocacy for improved RMNCAH services within the county since introduction of the Scorecard. They consider the RMNCAH Scorecard and its accompanying Action Tracker to be essential tools for increased coordination, service improvement, transparency and accountability in Bungoma County.
Regular civil society meetings are now held in the county through the Health NGO Network (HENNET) to ensure all non-government stakeholders in the health sector speak with ‘one voice’. Partners have further agreed that they will make their workplans public and ensure they are incorporated into the County’s Annual Work Plan. The partners have produced a number of joint advocacy products which have relied heavily on Scorecard data and gap analysis. These are credited with making a major contribution to increases in the county health budget.
The Scorecard has really attracted attention from implementing partners in the county and there’s continuing need to use it
Mr. Stephen Yambi, Project Director, E4A, MamaYe Project
400 traditional birth attendants
trained to become birth companions after scorecard analysis showed SBA was red
+30% in LLIN coverage for pregnant women
with key actions documented in the Action Tracker to resolve stockout bottlenecks
+25% in full immunisation coverage (FIC)
With implementation of key actions documented on the Action Tracker and support from partners
Improving quality of services
Quality of maternity service at PHC facilities has improved so much that, in 2014, a third of women delivered in lower level health facilities and two-thirds delivered in referral level facilities; whereas by 2018, the majority of women are now delivering in lower level facilities. This has significant efficiency gains for the county and families in terms of cost, as well as time away from home for the family. This change is attributed to a number of identified service gaps, affordability and accessibility issues prioritized during county and sub-county level RMNCAH Scorecard review meetings.
Future plans
- Intensify work to implement delayed actions (reduce the amount of red) in the Action Tracker
- Help HFs to access their respective scorecards digitally. Once a HF uses the digital RMNCAH Scorecard web platform, encourage them to also use the new workplan feature within the platform to save time and make their workplans more accessible for follow-up and accountability
- Explore the use of performance-based bonuses for CHVs or the introduction of income-generating activities
- Encourage additional relevant county TWGs to review and take actions related to the RMNCAH Scorecard since their membership includes other sectors with potential to impact health outcomes
- Work with the National MoH HMIS and other counties to address DHIS2 data configuration issues that relate to the national data platform and are not county-specific
- Foster incentives for data use and related actions. Reward those who take action as well as those who monitor and support the implementation of actions and provide vertical feedback to senior county officials.
Scorecard milestones
- 2017: RMNCAH Scorecard introduced, RMNCAH Task Force being established at county level
- 2018: Scorecard used at all MOH Levels in County. Health Facility Management Teams adjust Work Plans following SC reviews for targeted performance improvement
- 2019: SC data and trends are being used to establish priorities in upcoming Health Bill
- 2017 to 2019: County Health Budget significantly increases annually